Rotator Cuff Injuries
Irreparable Cuff Injuries
Irreparable tears involve chronic, massive tendon damage with severe retraction, muscle atrophy, and fatty infiltration. These tears cannot be repaired anatomically, even with mobilization. Treatment options focus on restoring function using alternative strategies, such as muscle advancement, tendon transfers, or biologic reconstruction. Management depends on patient age, activity level, and presence of arthritis.
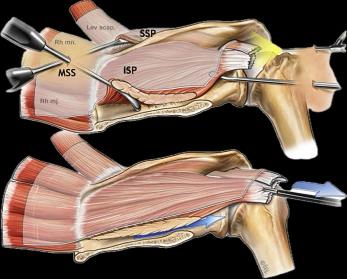
Muscle Advancement
Muscle advancement involves mobilizing and shifting the remaining rotator cuff muscles closer to the tuberosity to cover the defect. This is feasible in patients with partial retraction and good muscle bulk. It may be performed arthroscopically or with open techniques. While it doesn’t restore the exact anatomy, it can improve shoulder strength and function in selected cases. Muscle advancement is often combined with biologic augmentation (e.g., patch grafts) to reinforce the repair and reduce tension, especially in posterosuperior massive cuff tears.
Tendon Transfers – LTT, LD Transfers
Tendon transfers are used when native rotator cuff muscles are non-functional.
- Latissimus Dorsi (LD) Transfer is used primarily for irreparable posterosuperior tears in younger, active patients with intact deltoid function. It restores external rotation and overhead strength. It an also be used in massive irreparable subscapularis tears.
- Lower Trapezius Transfer (LTT) is a biomechanically favorable option for external rotation deficits, with poor postero-superior cuff tears. It better mimics the infraspinatus function and has gained popularity due to improved outcomes.
These procedures require precise technique and extensive rehabilitation but can significantly improve quality of life in appropriate candidates.
Superior Capsular Reconstruction (SCR)
SCR is an advanced arthroscopic technique that restores superior shoulder stability using a graft (usually fascia lata autograft or dermal allograft) placed between the glenoid and greater tuberosity. It prevents superior migration of the humeral head in irreparable supraspinatus tears. SCR is indicated in younger patients with preserved joint surfaces and functional deltoid. It allows pain relief and partial function restoration without joint replacement. Outcomes are promising when the graft is well-integrated and supported by intact subscapularis and infraspinatus. Proper rehabilitation focusing on passive motion and gradual strengthening is key to success.